A while ago, I mentioned that the cost of delaying lockdown by a week was to increase illness and death by a factor of 5, based on the doubling time of 3 days that the virus seemed to have at the start.
Human cost of delayed action – a short thread prompted by a tweet from @dougmcneall asking what the effect of a changing lockdown date (eg by a week) would be. Not long enough for a blog post! 1/— James Annan(@jamesannan) April 21, 2020
It’s a simple result but quite striking and perhaps counterintuitive, so here it is in more detail (and with slightly different numbers).
I’ve been fitting the SEIR epidemic model to the daily death data, and here is the latest hot-off-the-press version.

The magenta line is the median of my model fit, and the red circles are the data, though I have smoothed them a little to reduce the huge weekly cycle in reporting (Sun/Mon are always really low, then Tuesday really high).
This model allows the reproduction number to change at the lockdown date, and estimates the two values (which I call R0 and Rt) by fitting to the data. Taking that central magenta estimate, it is easy to re-run the model assuming the same change happened a week earlier. And this is what we get:
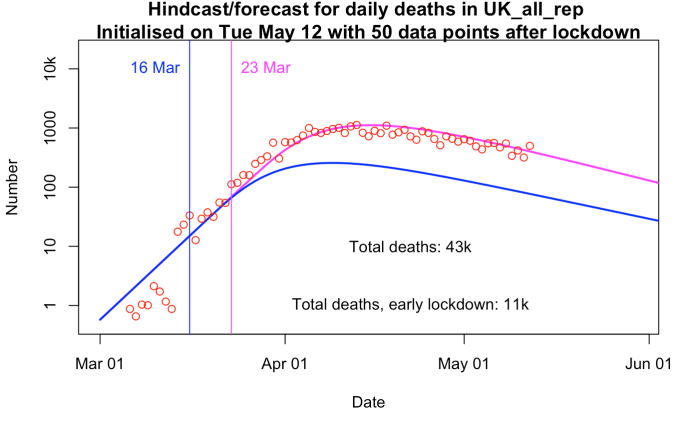
Magenta is as above, and blue is what happens if I make the change in R one week earlier, on the date of the blue vertical line. How did I know it would cause such a large reduction in deaths? The doubling time in the early phase is 3.5 days here (not 3 days as I got previously, told you the numbers were slightly different). So the size of the epidemic on this new lockdown date is exactly 1/4 the size it was on the later date. And the behaviour of exponentials (both growing and declining) is such that every day before or after the lockdown, the total size in the hypothetical case is also 1/4 what it was the same number of days before or after the lockdown in reality. The next plot shows this more clearly. I have just shifted the blue line forward by 1 week to make the lockdown dates coincide.

See the same shape, just lower? The logarithmic y-axis that I’m using means that a constant vertical distance between the solid blue and magenta lines corresponds to a constant ratio in numerical values, of 4 in this case. So the total number of deaths is also smaller by a factor of 4. The dashed blue line is the same model output as the solid blue line, only I’ve multiplied it by 4. You can see it overlies the original magenta almost exactly. Just towards the right hand edge of the graph there is a small mismatch, which is due to the magenta case benefiting from a slightly enhanced decline from a hint of the “herd immunity” phenomenon. That is to say, a with roughly 10% of the population having suffered from the disease in that scenario, these people (assumed to be immune) reduce the spread of the disease just enough for the lines to look a little bit different.
So, with these numbers that represent an initial doubling time of 3.5 days, we see that implementing the lockdown one week earlier would have saved about 30,000 lives in the current wave (based on official numbers, which are themselves a substantial underestimate). It would also have made for a shorter, cheaper, less damaging lockdown in economic terms. And this is all quite simple maths that every single modeller involved in SAGE was fully aware of at the time.
15 comments:
But this is only the first wave.
With an R0 around 3 the virus will eventually infect about 70% of the population and kill 1% of those infected.
The end point for the UK is 70% of 70 million infected, 49 million, and 490,000 dead.The
We stayed within the capacity of the NHS.
Unless we lose control, the outcome of the late lockdown was to bring some deaths forward from the second wave to the first wave, without affecting the final 490,000 total.
https://www.bbc.co.uk/programmes/m000j6ry
Disclosure: Scotlands Lockdown
Arrives at 80% fewer deaths, sounds somewhat familiar.
What took them so long? ;)
While a little extreme, I am thinking Entropic man has a bit of a point. How many have to have immunity for effective Rt to stay less than one with some social distancing but not lockdown?
Is the current effective Rt (including immunity effects) rather dominated by NHS and care home staff where immunity is rather higher than rest of population and if lockdown is eased not only does Rt increase due to less control measures but also because it circulates in population that is less immune?
Is there a need for more complex modelling that covers different populations?
Should we have one long lockdown until virus eliminated or should we come out early, have a second wave start then go back into lockdown and repeat until immunity levels high enough to stop virus spreading or something different?
On 16th March this report was given as advice to the UK government.
Download Report 9 here.
https://www.imperial.ac.uk/mrc-global-infectious-disease-analysis/covid-19/report-9-impact-of-npis-on-covid-19/
Look at Figure 4. It describes a long term strategy called adaptive triggering.
When R and caseload increase it triggers a tight lockdown. When cases drop it triggers easing of the lockdown. You might go through four or five cycles over 18 months as immunity gradually rises.
The aim is twofold.
1) Don't overload your health system. Extra people start dying on trollies are avoidable deaths.
2) Build towards herd immunity. This kicks in when enough people are immune and the virus finds it difficult to spread to new victims.
Our coronavirus has an Ro between 3 and 4. Herd immunity is effective when the proportion of the population immune exceeds 1-1/Ro. That is 66% to 75% of the population.
Lockdown early and keeping Rt low gives you a bunch of advantages. Endpoint may not be 70% infected - you might get vaccine to safely induce herd immunity. Also, you may get better treatment strategies, anti-virals etc to reduce IFR. Asian strategies of Stomp and Dance (test, contact trace and guarantine) so far seem to be working while economic life begins. We (NZ) opened most of economy (subject to social distancing) today. 3 days in row of zero new infections so stomp is working. Now to see well we can dance...
Indeed. Adaptive triggering buys time to develop a vaccine or other treatments. If a vaccine arrives quickly it saves a lot of lives. From my pessimistic viewpoint a vaccine in nine months would save 250,000 people in the UK alone. Death rates are also going down slightly with experience.
Unfortunately in the UK herd immunity requires about 50 million immune. WHO reckon that 6% of cases are reported. Thus our 5000 reported cases becomes a total of 83,000 cases per day. At that rate we reach herd immunity in 19 months, about when a vaccine is expected.
NZ is way ahead of the UK. You isolated and locked down very quickly and your isolation helped.
I hope your Stomp and Dance works. There are built in lags. It takes a week from infection to show symptoms, two weeks to need a hospital and three weeks to die, so your Rt data is always 1-3 weeks behind. Stomp and Dance might become WhackaMole.🤔
One other problem. Your population is not immune. You'll be like my wife, shielded in isolation until a vaccine comes.
NZ under 10 new confirmed cases a day since 18 April and only now coming out of lockdown but keeping social distancing! Under 10 per day seems a manageable dance so I am impressed that lockdown was kept for so long - perhaps it will be enough to eradicate in NZ.
I suspect other countries won't be so persistent and will be more concerned about their economy.
.
You missed the "with some social distancing but not lockdown" part of the question.
If R0 is 4 in unprepared and vulnerable population, but comes down to about 0.7 with lockdown, what R do you expect with lockdown ended but reasonably observed social distancing remaining?
If that is only 1.5 then 1-1/R only requires 33% to have immunity.
Is getting to this 33% faster while not overwhelming health system a "desirable outcome" because getting to this faster means it doesn't cost economy so much?
Rt with lockdown ended but with social distancing is very much dependent on how well the test, trace and quarantine works. (In effect dramatic "local" drop in Rt). I think "dance" does equal "whackamole". Wont end till have herd-immunity either by infection or vaccine. But it should keep Rt low and improving treatment options should keep death toll down too. Where do you get Rt of 0.7 with lockdown? With our severe 4 week lockdown, MoH estimated Rt as 0.4 from contact-tracing data whereas 4 before (from same data). 4 week total lockdown didnt seem too long compared what some have had to endure. (China was 8 weeks wasnt it).
We are about to see how well it works. 3 days in row without any new infections while stepping up survellience testing is a good start but we have seen how devastating just one undetected case can be. Getting the internal economy working now is aim, with hope that if the dance goes well, then we can open up to other countries who are also managing the dance well. July is the earliest that this could be even considered. Could all go pear-shaped but we will see.
>"Where do you get Rt of 0.7 with lockdown?"
From first image in James' post for the UK Rt=0.73+/- 0.08.
NZ clearly will follow plan to eliminate or keep as low as possible. Questions after . were a different topic for more heavily infected countries.
I can't see any politician in a democratic country following a policy to get to 33% of population infected as soon as possible unless they are practically there.
UK at 50,000 excess deaths vs 70m population * 33% * 0.7% IFR = ~160,000 deaths so could well be some way to go even in UK. (Unless R with some social distancing is more like 1.1 or less.)
"We stayed within the capacity of the NHS."
The NHS shut its doors to roughly half of all dying patients, sending them back into the community to spread infection further. If that's your definition of coping just fine, then sure, the NHS coped just fine. The victims may have a different view.
Yes. I've been using the basis % of ICU beds occupied measure. Put that way it's a very different story.
There may have been a certain amount of triage going on.
NICE suggested this point scale.
Athletic 1
Fit 2
Walking normally 3
Difficulty walking 4
Can't walk 5
Under 50 0
51-60 1
61-65 2
66-70 3
71-75 4
76-80 5
81+ 6
Underlying conditions 1 each
Terminal condition 9
Over 8 points, unlikely to survive Covid-19.
The scale was intended to be used when there were more cases than beds, to choose those more likely to survive, but it may have been used already to choose who to keep in hospital.
That raises a difficult dilemma. Do you keep a 10 pointer in a hospital bed blocking the admission of a 6 pointer; or do you send them back to the care home to spread the infection?
No win.
Keep the 10 pointer in hospital, they and the 6 pointer die. Send the 10 pointer back and they die, along with someone they infect.
Who would want that decision?
"If that is only 1.5 then 1-1/R only requires 33% to have immunity. "
But to keep that 33% herd immunity You have to keep the social distancing too.
The herd immunity might grow very slowly? Yes, social distancing fatigue could well be a bigger factor leading to a slight decline in infections slowly changing to growth in cases. If this takes time, taking us closer to point where we have a vaccine would this be more acceptable path than longer lockdown(s) which are surely more costly than just social distancing but longer lockdown would save more lives?
UK probably too far way from this point. Other places, Guayas? may be closer but not really have any choice: i.e. country can't afford a lockdown and too late so not really about choosing to pursue this policy.
"Take it on the chin" policy could possibly work at some level of acceptability if we slowly ramp up interaction starting with the least vulnerable and most economically valuable while protecting the elderly and avoiding an overload on healthcare at any one time. But if you're looking at another 100k deaths approx, then simple sums put that at 200 days of 500 per day which is a hell of a long haul before we are back to anything near normal. And the vulnerable need to be able to access health services safely during this time, which has been a real problem. It's not enough to just tell them to stay at home. Routine check-ups, cancer, all the rest. Segregating covid cases into new nightingale hospitals would be a start, then perhaps hospitals could be cleaned up. Currently they are deathtraps.
There's just not an attractive route out without some extremely good luck along the way - whether that be a strong summer effect, an early vaccine, or the govt pulling its finger out and doing a spectacular job on TTI.
(Don't forget the I - without rigorous isolation, all the testing in the world doesn't do any good.)
Post a Comment